
At some point, we may have made a trip to the clinic and as part of the examination, the clinician pulls out a device and listens to your lungs, but what do they actually listen for?
Auscultation is the act of listening to sounds made by internal organs and vessels of the human body. This is usually done with a device called a stethoscope. It is a technique used to examine the respiratory system (breath sounds), cardiovascular system (heart sounds and vascular bruits) and gastrointestinal system (bowel sounds).
It is a vital part of the respiratory examination as it can be used to identify certain diseases based on abnormal breath sounds.
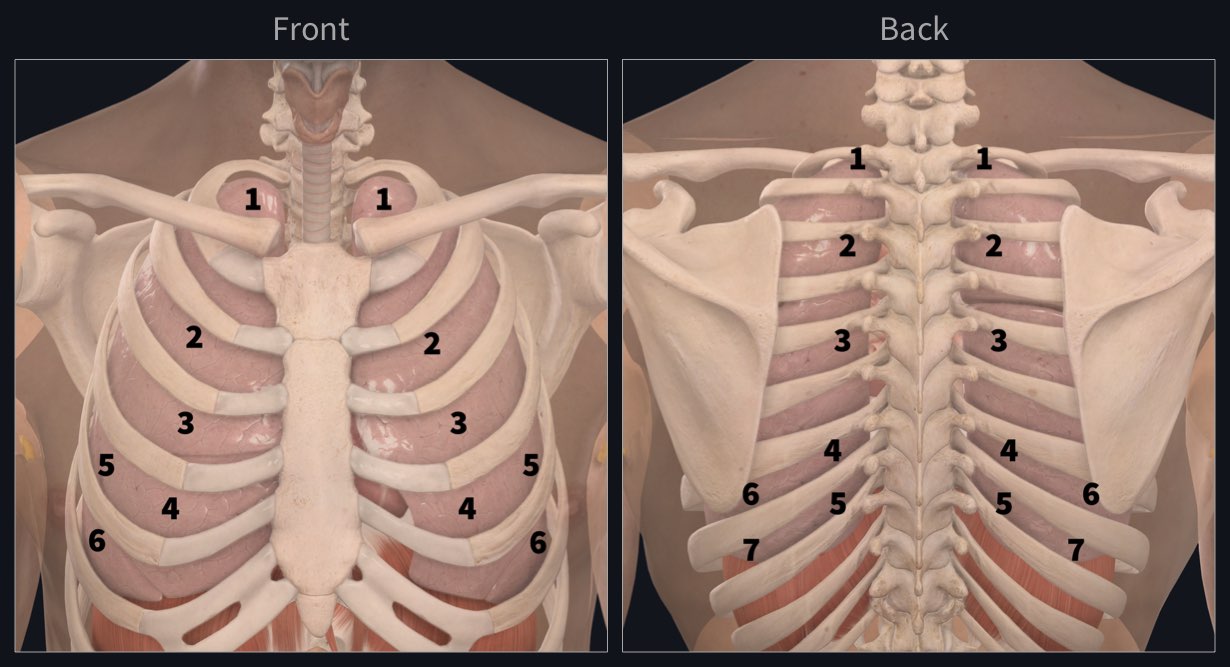
The clinician can identify the exact location of the auscultation points on the patient through the combined knowledge of surface anatomy, the skeleton and the main lobes of the lungs. Although surface markers do not always give an exact relationship of underlying structures, they do give a sufficiently accurate gauge of what lies beneath the skin.
The right lung is divided into 3 main lobes which are separated by the oblique and horizontal fissures. These lobes are: the superior, middle and inferior lobes. The left lung is separated by the oblique fissure into 2 main lobes: the superior and inferior.
During auscultation, the clinician listens for abnormal breath sounds in these lobes by placing the stethoscope at particular areas on each side of the patient’s chest wall and back. The clinician will move in a zig-zag pattern, moving back and forth from one side of the body to the other, as they work their way down the chest and back.
They will ask the patient to take deep breaths in and out and as air flows in and out of the lungs, any abnormal breath sounds will be picked up by the clinician.
There are 3 main characters of breath sounds and they include:
- Quality: A normal breath sound (vesicular breath sound) should not have any additional sounds
- Volume: Quiet or decreased breath sounds suggest reduced air entry into the lungs which may be as a result of fluid in the lungs or an infection.
- Added sounds: Such as wheezes (asthma and COPD) and crackles ( pneumonia or fluid overload).
Identify the points of auscultation with the world’s most accurate and advanced 3D anatomy atlas. Try it for FREE today.
If you found this blog post useful, you might also enjoy learning about the blood supply to the lung.
